吉林大学学报(医学版) ›› 2021, Vol. 47 ›› Issue (5): 1273-1280.doi: 10.13481/j.1671-587X.20210527
生长发育期骨性Ⅱ类错 畸形儿童上气道矢状径主要影响因素分析
畸形儿童上气道矢状径主要影响因素分析
陆晨萌,张祎,尹茂运,米合日扎提·买买提,刘新煜,胡敏( )
)
- 吉林大学口腔医院正畸科,吉林 长春 130021
Analysis on main factors affecting sagittal diameter of upper airway in children with skeletal class Ⅱ malocclusion during growth and development period
Chenmeng LU,Yi ZHANG,Maoyun YIN,Mamat MIHRIZAT,Xinyu LIU,Min HU()
- Department of Orthodontics,Stomatology Hospital,Jilin University,Changchun 130021,China
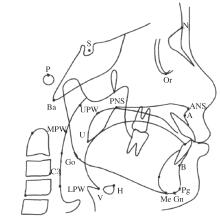
摘要: 探讨影响生长发育期骨性Ⅱ类错 选取2017—2018年就诊于本院正畸科9~15岁生长发育期骨性Ⅱ类错 在喉咽段,与QCVMⅠ-Ⅱ期比较,喉咽段气道矢状径(V-LPW)在QCVMⅡ-Ⅲ期、Ⅲ-Ⅳ期明显增大;在鼻咽段,与QCVMⅠ-Ⅱ期、Ⅲ-Ⅳ期比较,鼻咽腔气道矢状径(PNS-UPW)在QCVMⅡ-Ⅲ期增大(P<0.05)。在喉咽段,喉咽腔气道矢状径(V-LPW)随体质量指数(BMI)的增大而增大,在低体质量组与正常组、低体质量组与超重组间比较差异有统计学意义(P<0.05)。低体质量组患儿鼻咽腔和下口咽腔气道段矢状径(PNS-UPW和U-MPW)低于正常组(P<0.05)。在鼻咽气道,蝶鞍点-鼻根点-下齿槽座点(SNB)和患儿是否处于QCVMⅡ期是PNS-UPW的影响因素(P<0.05);在口咽气道,舌骨前下点距第三颈椎前下点距离(H-C3)、上齿槽座点-鼻根点-下齿槽座点(ANB)和软腭长度(SPL)是U-MPW的影响因素(P<0.05);在喉咽气道,H-C3和患儿是否为低体质量是V-LPW的影响因素(P<0.05);在下口咽气道间隙,H-C3、ANB和患儿是否为低体质量是下口咽气道间隙(PAS)的影响因素(P<0.05)。 生长发育期骨性Ⅱ类错 畸形儿童上气道矢状径的相关因素,为临床包含气道预测的正畸方案的制定提供思路。
畸形儿童上气道矢状径的相关因素,为临床包含气道预测的正畸方案的制定提供思路。 畸形儿童共100例,进行回顾性研究。收集患儿一般信息(性别、身高和体质量)、牙弓测量数据和X线头影测量分析数据,分析生长发育期骨性Ⅱ类错
畸形儿童共100例,进行回顾性研究。收集患儿一般信息(性别、身高和体质量)、牙弓测量数据和X线头影测量分析数据,分析生长发育期骨性Ⅱ类错 畸形儿童上气道矢状径情况,通过逐步回归分析得出影响上气道各段矢状径大小的相关因素。
畸形儿童上气道矢状径情况,通过逐步回归分析得出影响上气道各段矢状径大小的相关因素。 畸形儿童上气道矢状径与周围软硬组织关系密切,在制定临床正畸治疗方案时需要全面评估上气道与患儿自身状况,避免医源性因素造成患儿上气道阻塞,同时为预后提供参考依据。
畸形儿童上气道矢状径与周围软硬组织关系密切,在制定临床正畸治疗方案时需要全面评估上气道与患儿自身状况,避免医源性因素造成患儿上气道阻塞,同时为预后提供参考依据。
中图分类号:
- R783.5

 畸形患病率的调查[J]. 中华口腔医学杂志, 2002, 37(5): 371-373
畸形患病率的调查[J]. 中华口腔医学杂志, 2002, 37(5): 371-373 青少年上下颌骨垂直向及纵向变化的研究[J]. 临床口腔医学杂志, 2010, 26(6): 326-329.
青少年上下颌骨垂直向及纵向变化的研究[J]. 临床口腔医学杂志, 2010, 26(6): 326-329.