吉林大学学报(医学版) ›› 2022, Vol. 48 ›› Issue (3): 796-800.doi: 10.13481/j.1671-587X.20220330
• 临床医学 • 上一篇
以肺部影像学改变为首发表现的血管免疫母细胞性T细胞淋巴瘤1例报告及文献复习
李倩,苑静怡,周佳奇,赵敏,王珂( )
)
- 吉林大学第二医院呼吸与危重症医学科,吉林 长春 130041
Pulmonary imaging changes as first manifestation of angioimmunoblastic T-cell lymphoma: A case report and literature review
Qian LI,Jingyi YUAN,Jiaqi ZHOU,Min ZHAO,Ke WANG()
- Department of Respiratory and Critical Care Medicine,Second Hospital,Jilin University,Changchun 130041,China
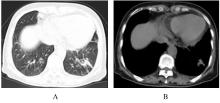
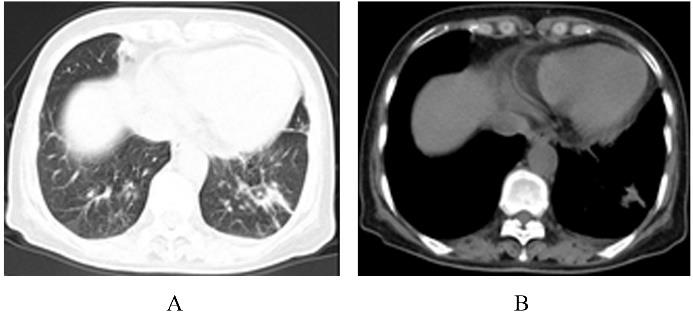
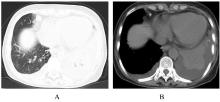
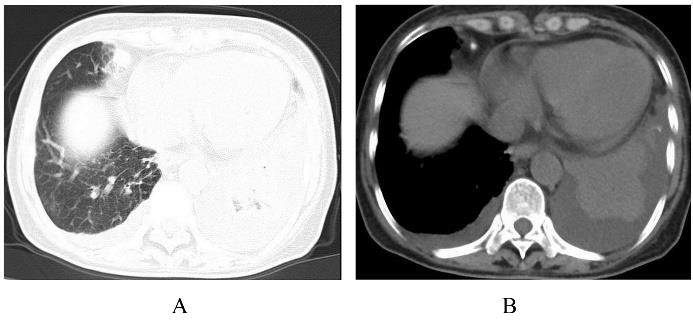
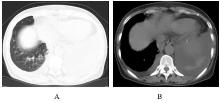
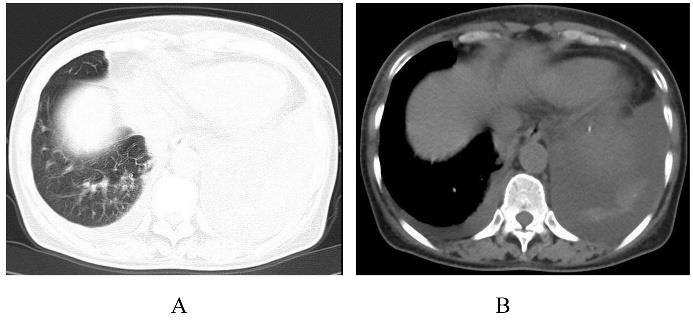
摘要: 探讨血管免疫母细胞性T细胞淋巴瘤(AITL)的临床特点、诊断过程和治疗方法,提高临床医生对该病的认识。 收集1例AITL患者的临床资料、影像学表现、支气管镜和病理检查结果,分析上述资料,并进行相关文献复习。 患者,女性,66岁,因“发热伴咳嗽和咳痰15 d”入院。患者四肢散在红色皮疹,胸廓无畸形,气管居中,叩诊左下肺浊音,左下肺呼吸音减弱,无其他明显阳性体征。胸部CT检查结果显示双肺下叶见多发条片状高密度影,以左下肺为著,纵隔和双侧腋窝淋巴结肿大。初步考虑双肺炎症可能性大,待除外占位性病变。经支气管镜肺活检术(TBLB)、纵隔淋巴结支气管穿刺针吸活检术(TBNA)和胸水脱落细胞检测,结果均排除肺恶性病变。先后行抗感染治疗和实验性抗结核治疗,患者仍反复发热,多次复查胸部CT结果显示左下肺高密度影范围增大和实变。全面的实验室检查和影像学检查均未见异常,患者具体发热原因不明确。患者查体见躯干和四肢多发淡红色皮疹,双侧锁骨上淋巴结肿大,经右侧锁骨上淋巴结穿刺活组织检查,最终病理回报AITL。 有肺部影像学改变的不明原因发热,且伴有皮疹及淋巴结肿大的患者,如系统抗感染治疗效果不好,应考虑AITL。
中图分类号:
- R733.4