吉林大学学报(医学版) ›› 2026, Vol. 52 ›› Issue (2): 530-535.doi: 10.13481/j.1671-587X.20260226
呈黄褐混浊态的双侧胸腔积液快速交替进展患者1例报告及文献复习
丁艺,贾文慧,杨晨露,董春玲( )
)
- 吉林大学第二医院呼吸与危重症医学科,吉林 长春 130041
Bilateral pleural effusion with rapid alternating progression in patient with yellow-brown turbid appearance:A case report and literature review
Yi DING,Wenhui JIA,Chenlu YANG,Chunling DONG()
- Department of Respiratory and Critical Care Medicine,Second Hospital,Jilin University,Changchun 130041,China
摘要:
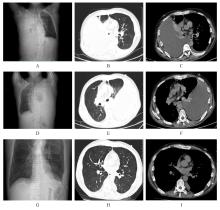
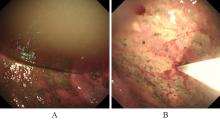
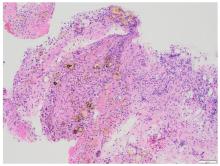
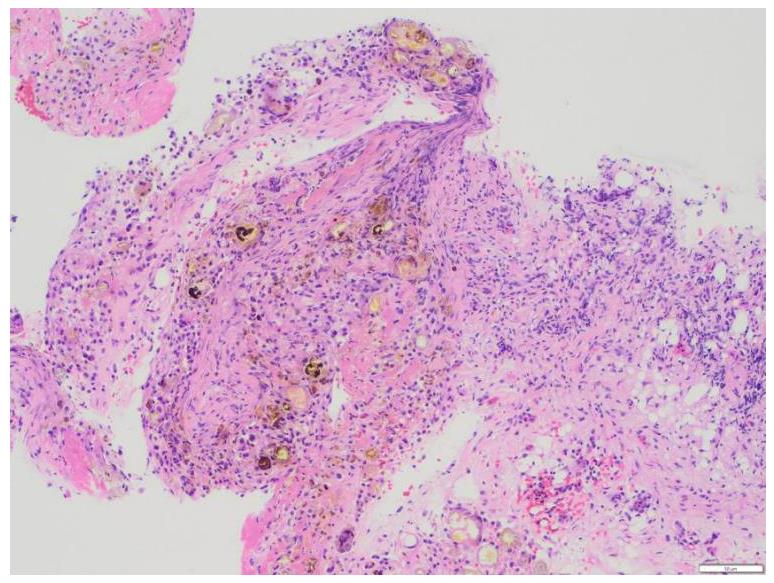
胰源性胸腔积液常由胰腺假性囊肿、胰胸膜瘘(PPF)和胰腺炎等引发。该疾病的临床表现以胸部症状为主,腹部症状较少见,缺乏特异性,故极易出现诊治延误。呈黄褐混浊态的双侧胸腔积液快速交替进展者较为罕见,国内外未见相关报道。本文作者报道1例胰源性胸腔积液患者,对其临床表现、胸膜病理特点及诊治方案进行总结,并结合相关文献进行复习。患者,男性,40岁,因“咳嗽、咳痰、胸痛伴阵发性呼吸困难”就诊,其胸腔积液呈快速进展的黄褐混浊态,排查常见病因后未能明确诊断,治疗期间突发腹痛。结合患者既往有长期饮酒史并曾行胰腺假性囊肿胃吻合术,遂完善胸腔积液淀粉酶检查,明确诊断继发于胰腺假性囊肿的胰源性胸腔积液,并行内镜逆行胰胆管造影(ERCP)及相关介入治疗。定期随访后,胸腔积液无复发迹象。对于有胰腺相关病史的胸腔积液患者,无论是否并发腹部症状,均应考虑胰源性胸腔积液的可能,并警惕血胸、脓胸、纵隔炎和呼吸衰竭等相关严重并发症。对于内科治疗效果不佳者,应细致评估胰液引流路径及解剖异常,以指导精准个体化治疗,改善患者预后。
中图分类号:
- R561.3


 并发舌体肥大1例报告及文献复习
并发舌体肥大1例报告及文献复习