Journal of Jilin University(Medicine Edition) ›› 2026, Vol. 52 ›› Issue (2): 530-535.doi: 10.13481/j.1671-587X.20260226
• Clinical medicine • Previous Articles Next Articles
Bilateral pleural effusion with rapid alternating progression in patient with yellow-brown turbid appearance:A case report and literature review
Yi DING,Wenhui JIA,Chenlu YANG,Chunling DONG( )
)
- Department of Respiratory and Critical Care Medicine,Second Hospital,Jilin University,Changchun 130041,China
-
Received:2025-06-02Accepted:2025-07-14Online:2026-03-28Published:2026-04-15 -
Contact:Chunling DONG E-mail:cldong@jlu.edu.cn
CLC Number:
- R561.3
Cite this article
Yi DING,Wenhui JIA,Chenlu YANG,Chunling DONG. Bilateral pleural effusion with rapid alternating progression in patient with yellow-brown turbid appearance:A case report and literature review[J].Journal of Jilin University(Medicine Edition), 2026, 52(2): 530-535.
share this article
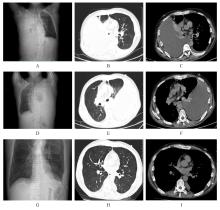
Fig. 1
Chest CT images of patients with bilateral pleural effusion"
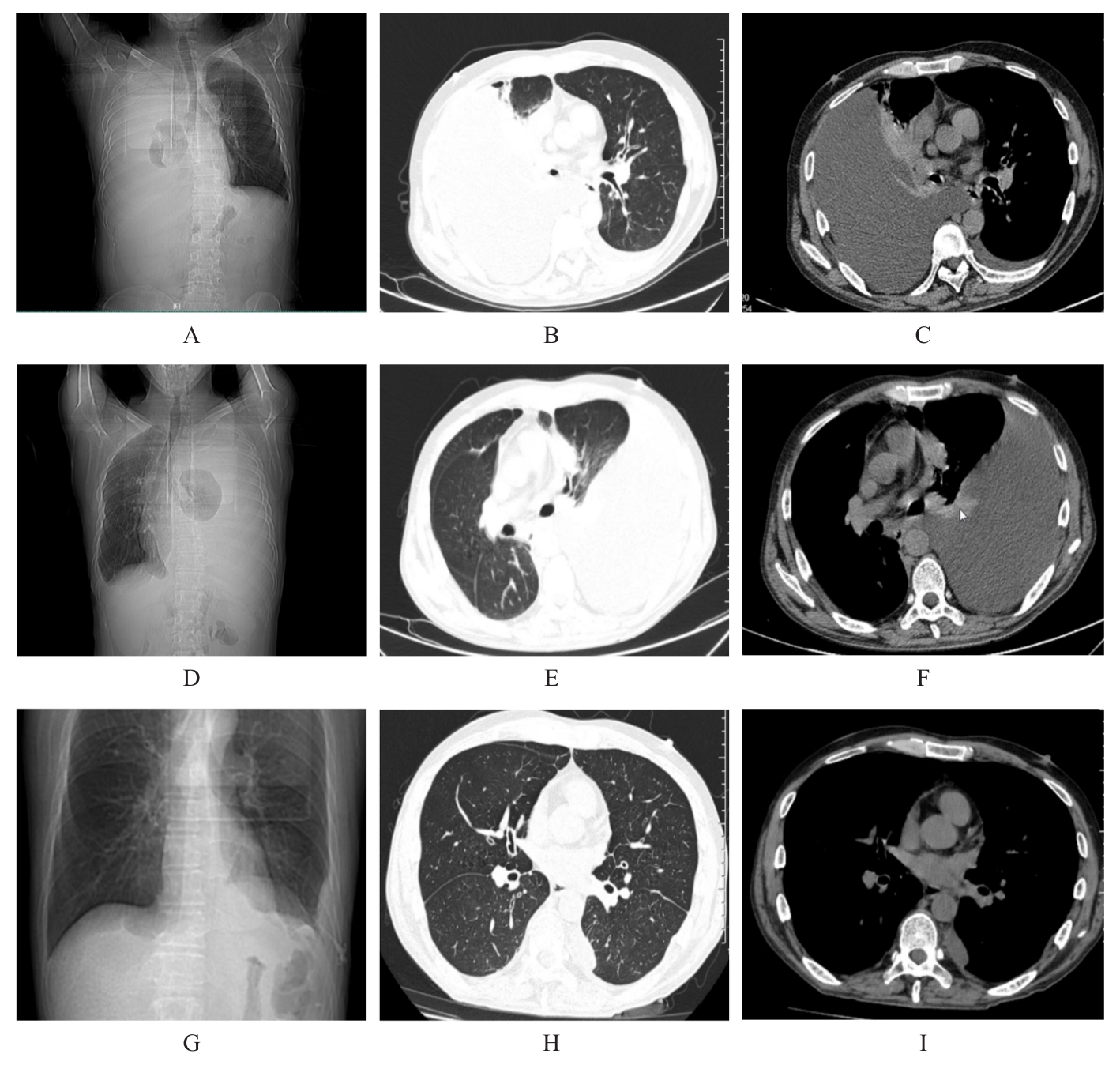
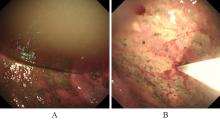
Fig. 2
Chest endoscope findings of patient with bilateral pleural effusion"
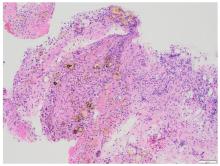
Fig. 3
Pathomorphology of right parietal pleural biopsy tissue of patient with bilateral pleural effusion(HE,×40)"
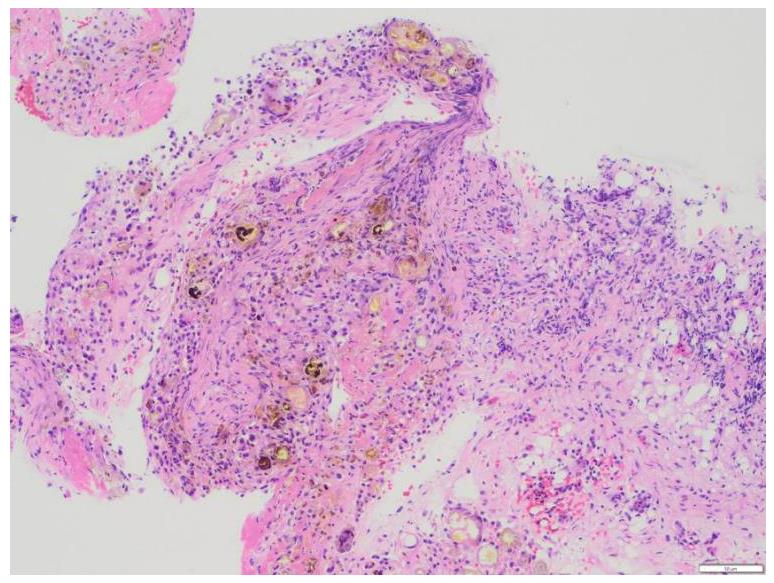

Fig. 4
Abdominal CT image of patient with bilateral pleural effusion"

| [1] | 中华医学会呼吸病学分会胸膜与纵隔疾病学组(筹). 胸腔积液诊断的中国专家共识[J]. 中华结核和呼吸杂志,2022, 45(11): 1080-1096. |
| [2] | LIGHT R W. Pleural effusions[J]. Med Clin N Am, 2011, 95(6): 1055-1070. |
| [3] | 吴 迪, 刘盛国, 杨 凯, 等. 胸腔积液的病因分布及临床特点[J]. 广东医学, 2020, 41(14): 1459-1463. |
| [4] | TIAN P W, QIU R, WANG M F, et al. Prevalence, causes, and health care burden of pleural effusions among hospitalized adults in China[J]. JAMA Netw Open, 2021, 4(8): e2120306. |
| [5] | COELHO M N, BASTO T, ALMEIDA J, et al. Pancreaticopleural fistula as the inaugural presentation of chronic pancreatitis: a case report[J]. Int J Surg Case Rep, 2024, 119: 109755. |
| [6] | KABAY K, BRYCE G. Pancreaticopleural fistula: a rare aetiology of pleural effusion[J]. BMJ Case Rep, 2024, 17(12): e261933. |
| [7] | MURTEIRA F, COSTA T, PINTO S B, et al. Pancreaticopleural fistula: an insidious cause of pleural effusion-case report[J]. J Cardiovasc Thorac Res, 2022, 14(1): 67-70. |
| [8] | SALGUERO B, KAKKED G, NARAYANSWAMI G, et al. Characteristics and management of pancreatic pleural effusions: a systematic review of case reports[J]. Chest, 2018, 154(4): 513A. |
| [9] | 王薇, 刘丽平. 以血性胸腔积液首发的儿童胰腺胸膜瘘1例报告并文献复习[J]. 中国实用儿科杂志, 2021, 36(3): 231-234. |
| [10] | KOLIAKOS N, PAPACONSTANTINOU D, TZORTZIS A S, et al. Endoscopic versus surgical treatment for thoracopancreatic fistulas complicating chronic pancreatitis: a systematic review[J]. Surgery, 2022, 171(5): 1373-1378. |
| [11] | EDDERY R, SEARLE L, IQBAL M, et al. Pleural effusion in a patient with previous alcohol excess[J]. Breathe, 2024, 20(2): 240036. |
| [12] | 何 亮, 钟一丹, 马文燕, 等. 胰胸膜瘘致大量胸腔积液1例[J]. 临床肺科杂志, 2023, 28(7): 1123-1125. |
| [13] | LIU R X, SU R L, YAN H Y, et al. Pancreaticopleural fistula causing recurrent bilateral pleural effusions: a case report[J]. Medicine, 2024, 103(51): e41029. |
| [14] | 刘峰辉, 刘艳君, 罗振宇, 等. 黑色胸腔积液1例报告并文献复习[J]. 青岛大学学报(医学版), 2022, 58(5): 777-780. |
| [15] | 韩文雅, 任 涛, 喻志芳, 等. 慢性胰腺炎并发大量胸腔积液1例报道并文献复习[J]. 临床肺科杂志, 2023, 28(6): 970-972. |
| [16] | KHADKA M, BHUSAL S, PANTHA B, et al. Pancreaticopleural fistula causing pleural effusion: a case report and review of the literature[J]. J Med Case Rep, 2024, 18(1): 131. |
| [17] | LARSEN M, KOZAREK R. Management of pancreatic ductal leaks and fistulae[J]. J Gastroenterol Hepatol, 2014, 29(7): 1360-1370. |
| [18] | SALEH Z, PAWAR R, PILLAI A, et al. Pancreatitis as a pulmonary pathology: a rare case of a pancreaticopleural fistula presenting as recurrent pleural effusions causing mediastinal shift[J]. Cureus, 2024, 16(7): e64246. |
| [19] | DHEBRI A R, FERRAN N. Nonsurgical management of pancreaticopleural fistula[J]. JOP, 2005, 6(2): 152-161. |
| [20] | 柴宁莉, 杜晨, 翟亚奇, 等. 中国胰瘘消化内镜诊治专家共识(2020, 北京)[J]. 中华胃肠内镜电子杂志, 2020, 7(3): 97-107. |
| [21] | BOLDIN B V, PONOMAR S A, REVYAKIN V I. Pancreaticopleural fistula is a possible cause of acute respiratory failure[J]. Khirurgiia, 2018(5): 115-116. |
| [22] | KOKHANENKO N Y, KASHINTSEV A A, BOBYLKOV A A, et al. Staged interventional and surgical treatment of patient with chronic pancreatitis complicated by pancreaticopleural fistula with lung abscesses[J]. Am J Case Rep, 2020, 21: e922195. |
| [23] | 皮之安, 朱亚男, 周和平, 等. 多学科联合诊断胰腺胸膜瘘病例报道1例[J]. 中华胸部外科电子杂志, 2021, 8(3): 186-189. |
| [1] | Zhongwei ZHOU,Wei DU,Yu NING,Jing YU,Fengyou GUO,Xueliang YANG. SMARCB1/INI1-deficient undifferentiated pancreatic carcinoma: A case report and literature review [J]. Journal of Jilin University(Medicine Edition), 2026, 52(2): 523-529. |
| [2] | Lei TIAN, Yuyan LIU, Yuqing WANG, Zhiyu ZHANG, Xiumei SUN. Grade Ⅲ open bite complicated with tongue hypertrophy treated by mandibular incisor extraction:A case report and literature review [J]. Journal of Jilin University(Medicine Edition), 2026, 52(1): 236-245. |
| [3] | Shuangji LI,He SHI,Yiwen QIN,Xiang LI,Yuyang LI,Weiwei LIU,Jia LI. Desmoplastic fibroma of mandible: A case report and literature review [J]. Journal of Jilin University(Medicine Edition), 2026, 52(1): 246-251. |
| [4] | Lei SUN,Yong YU,Xiaojun LIU,Sheng MIAO. 46, XX male sex reversal syndrome:A case report and literature review [J]. Journal of Jilin University(Medicine Edition), 2026, 52(1): 252-256. |
| [5] | Yi LIU,Qingguang MENG, Hugejile,Yang QU. Spinal gout patient with intervertebral disc involvement and nerve compression treated with unilateral biportal endoscopic surgery: A case report and literature review [J]. Journal of Jilin University(Medicine Edition), 2026, 52(1): 257-263. |
| [6] | Qian AO,Jingting LI,Nan LIANG,Hui SUN. Recurrent follicular variant of papillary thyroid carcinoma with DICER1 mutation in adolescent:A case report and literature review [J]. Journal of Jilin University(Medicine Edition), 2025, 51(6): 1702-1708. |
| [7] | Pengqing WU,Lingpeng ZENG,Zhaoxia LUO,Yangyang LEI,Ruiqin GOU,Qing ZHANG. Thymus physiological uptake in patient with differentiated thyroid carcinoma after postoperative iodine-131 treatment: A case report and literature review [J]. Journal of Jilin University(Medicine Edition), 2025, 51(5): 1358-1362. |
| [8] | Geer A,Qin WANG,Lijing JIAO,Hailun ZHOU,Shanshan GAN,Yang HAN,Ruichao LIU,Yabin GONG. Research progress in effects of CD4+T cell-mediated immune tolerance on occurrence and development of malignant pleural effusion [J]. Journal of Jilin University(Medicine Edition), 2025, 51(4): 1121-1128. |
| [9] | Xiangjin HU,Xiumei SUN,Kai CHEN,Guomin WU. Changes of upper airway in patient with skeletal class Ⅱ malocclusion accompanied by OSAHS after maxillomandibular advancement surgery: A case report and literature review [J]. Journal of Jilin University(Medicine Edition), 2025, 51(2): 493-500. |
| [10] | Qi ZHANG,Xiaoyuan XU,Yumiao WU,Han ZHANG,Zhiqiang HU,Jiamin YUAN,Yuchen CUI,Xianchun ZHU. Treatment of skeletal class Ⅱ high angle malocclusion patient by clear aligner therapy combined with orthognathic surgery: A case report and literature review [J]. Journal of Jilin University(Medicine Edition), 2025, 51(2): 508-515. |
| [11] | Luyao WANG,Chenxi ZHAO,Wanze ZHANG,Linlin LIU. Second primary tracheal adenoid cystic carcinoma:A case report and literature review [J]. Journal of Jilin University(Medicine Edition), 2025, 51(1): 215-221. |
| [12] | Jinping ZHANG,Lingling TONG,Lu GAO,Hongjing CHENG,Minjia SHENG. Parasitic leiomyoma of abdominal wall complicated with disseminated peritoneal leiomyomatosis : A case report and literature review [J]. Journal of Jilin University(Medicine Edition), 2024, 50(5): 1432-1437. |
| [13] | Wenqing RUAN,Zerun FU,Yi HUANG,Longyun LI,Yao SUN,Kai LI. Application of hypotension prediction index in intraoperative hemodynamic management of robot-assisted laparoscopic cystectomy:A case report and literature review [J]. Journal of Jilin University(Medicine Edition), 2024, 50(4): 1130-1136. |
| [14] | Shaoning KAN,Han WU,Shuangji LI,Jingcheng XIANG,Yuyang LI,Liou JIN,Weiwei LIU. Simple bone cyst in ipsilateral maxilla and mandible:A case report and literature review [J]. Journal of Jilin University(Medicine Edition), 2024, 50(2): 551-555. |
| [15] | Qinghua PING,Wenjing ZHU,Jianxin XIA. Pustular psoriasis treated with secukinumab during pregency: A case report and literature review [J]. Journal of Jilin University(Medicine Edition), 2023, 49(6): 1599-1603. |