吉林大学学报(医学版) ›› 2023, Vol. 49 ›› Issue (6): 1593-1598.doi: 10.13481/j.1671-587X.20230624
超声诊断十二指肠后壁穿孔致胆囊周围积液1例报告及文献复习
朱晴,吴明丽,刘琦尧,张镰竞,胡月,杨冬艳( )
)
- 吉林大学中日联谊医院超声科,吉林 长春 130033
Ultrasonographic diagnosis of peri-gallbladder fluid caused by posterior duodenal perforation:A case report and literature review
Qing ZHU,Mingli WU,Qiyao LIU,Lianjing ZHANG,Yue HU,Dongyan YANG()
- Department of Ultrasonography,China-Japan Union Hospital,Jilin University,Changchun 130033,China
摘要:
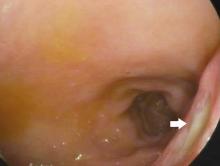
目的 分析1例由超声首诊的十二指肠后壁穿孔导致胆囊周围积液患者的影像学表现及其临床诊断和治疗经过,为该病的临床诊断提供依据。 方法 收集1例十二指肠后壁穿孔导致胆囊周围积液患者的临床资料、实验室检查、胃镜和影像学表现,记录其诊疗过程并进行随访。结合相关文献复习,分析十二指肠后壁穿孔的临床特点和影像学表现。 结果 患者,男性,50岁,无明显诱因右上腹持续性钝痛超过20 d、餐后加剧,同时伴有右腰背部放射性疼痛,于当地医院行超声检查提示胆囊占位性病变,为求进一步诊治就诊于本院。入院当日行腹部超声检查,可见空腹胆囊充盈极差,囊壁连续且弥漫均匀增厚,胆囊腔内见多发强回声,胆囊周围可见杂乱分布的无及弱回声延续至十二指肠球部后方,与球部以窄条状气体影相通。超声考虑为十二指肠球部后壁穿孔导致胆囊周围积液,胆囊受压充盈极差,胆囊壁慢性炎症改变伴胆囊结石。计算机断层扫描(CT)增强检查可见十二指肠球部后壁穿孔处清晰显示,CT结论与超声结论相似;胃镜检查显示十二指肠球部后壁深大溃疡,证实诊断为溃疡穿孔导致胆囊周围积液。置入胃管和空肠营养管,同时行消炎、镇痛和抑酸等对症治疗,治疗3个月内复查超声显示胆囊周围积液逐渐减少、胆囊腔逐渐充盈。患者因胆囊炎症状持续存在,遂行胆囊切除术,病理诊断为慢性胆囊炎并发胆囊结石。 结论 十二指肠后壁穿孔常因临床表现不典型而导致误诊或漏诊,影像学检查可辅助临床进行早期诊断,在腹部气体干扰未影响观察时,超声可作为消化道穿孔首选且有效的诊断方法。
中图分类号:
- R575.63