Journal of Jilin University(Medicine Edition) ›› 2022, Vol. 48 ›› Issue (6): 1510-1517.doi: 10.13481/j.1671-587X.20220617
• Research in clinical medicine • Previous Articles Next Articles
Clinicopathological characteristics and analysis on prognostic factors of patients with solitary fibrous tumors in different sites
Yunhe GAO,Jianan YAO,Lanqing CAO,Chuanjie XU( )
)
- Department of Pathology,Second Hospital,JilinUniversity,Changchun 130041,China
-
Received:2022-01-22Online:2022-11-28Published:2022-12-07 -
Contact:Chuanjie XU E-mail:xucj@jlu.edu.cn
CLC Number:
- R73
Cite this article
Yunhe GAO,Jianan YAO,Lanqing CAO,Chuanjie XU. Clinicopathological characteristics and analysis on prognostic factors of patients with solitary fibrous tumors in different sites[J].Journal of Jilin University(Medicine Edition), 2022, 48(6): 1510-1517.
share this article
Tab. 1
Clinicopathological data of 86 SFT patients"
| Pathogenic site | n | Gender constituentratio (Male: female) | Age (years) | Diameter (l/cm) | Mitotic count (/10 HPF) | No.of associated necrosis | No.of low-risk | No.ofmedium-risk | No.of high-risk | Follow-up time (month) | No.of recurrence |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Central nervous system | 5 | 4∶1 | 44.60±14.12 | 4.70±2.01 | 1.40±0.55 | 0 | 5 | 0 | 0 | 26-29 | 0 |
| Female genital tract | 8 | 0∶8 | 50.09±14.22 | 59.69±4.89 | 3.25±2.87 | 3 | 4 | 3 | 1 | 2-95 | 3 |
| Abdominal neoplasm | 11 | 3∶8 | 49.45±17.06 | 12.36±9.40 | 3.45±3.80 | 2 | 6 | 2 | 3 | 11-67 | 2 |
| Upper respiratory tract | 11 | 4∶7 | 57.36±14.49 | 3.18±1.31 | 2.00±2.05 | 0 | 11 | 0 | 0 | 13-139 | 0 |
| Subcutaneous soft tissue | 11 | 5∶6 | 50.09±12.23 | 6.32±4.37 | 2.82±2.27 | 2 | 8 | 2 | 1 | 7-96 | 2 |
| Orbit | 16 | 8∶8 | 54.94±19.15 | 2.31±1.16 | 3.25±2.86 | 0 | 15 | 1 | 0 | 3-98 | 1 |
| Lung and pleura | 24 | 13∶11 | 57.96±12.56 | 8.93±3.12 | 3.33±3.12 | 4 | 16 | 6 | 2 | 7-109 | 2 |

Fig. 1
General morphology of SFT"
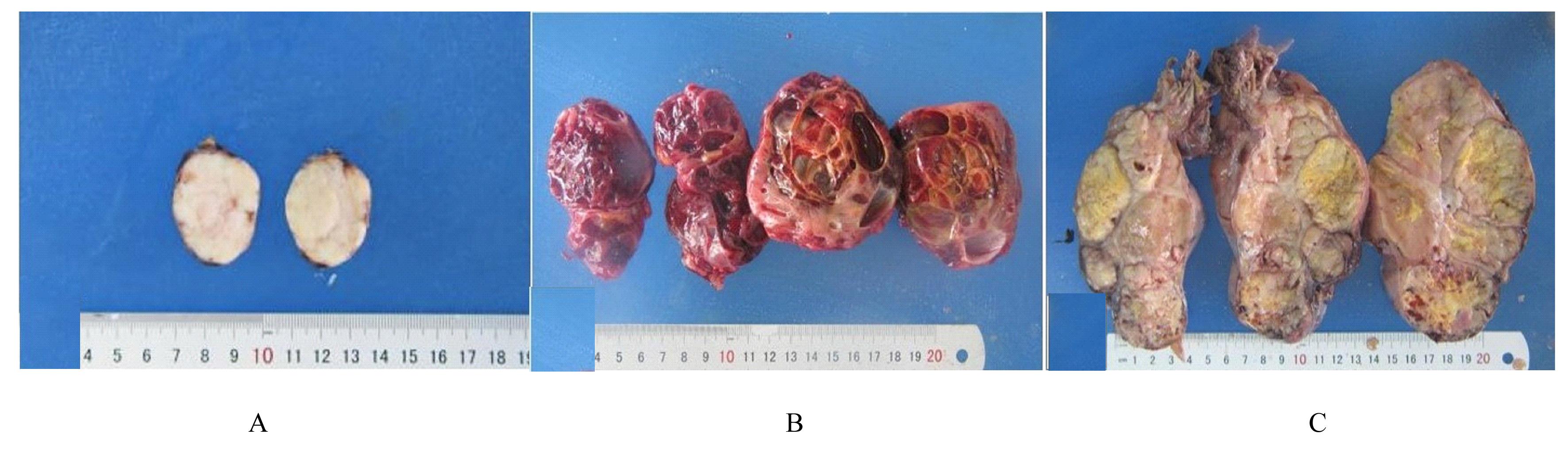

Fig. 2
Morphology of SFT under microscope observed by HE staining"


Fig. 3
Immunohistochemical staining detection results of SFT"


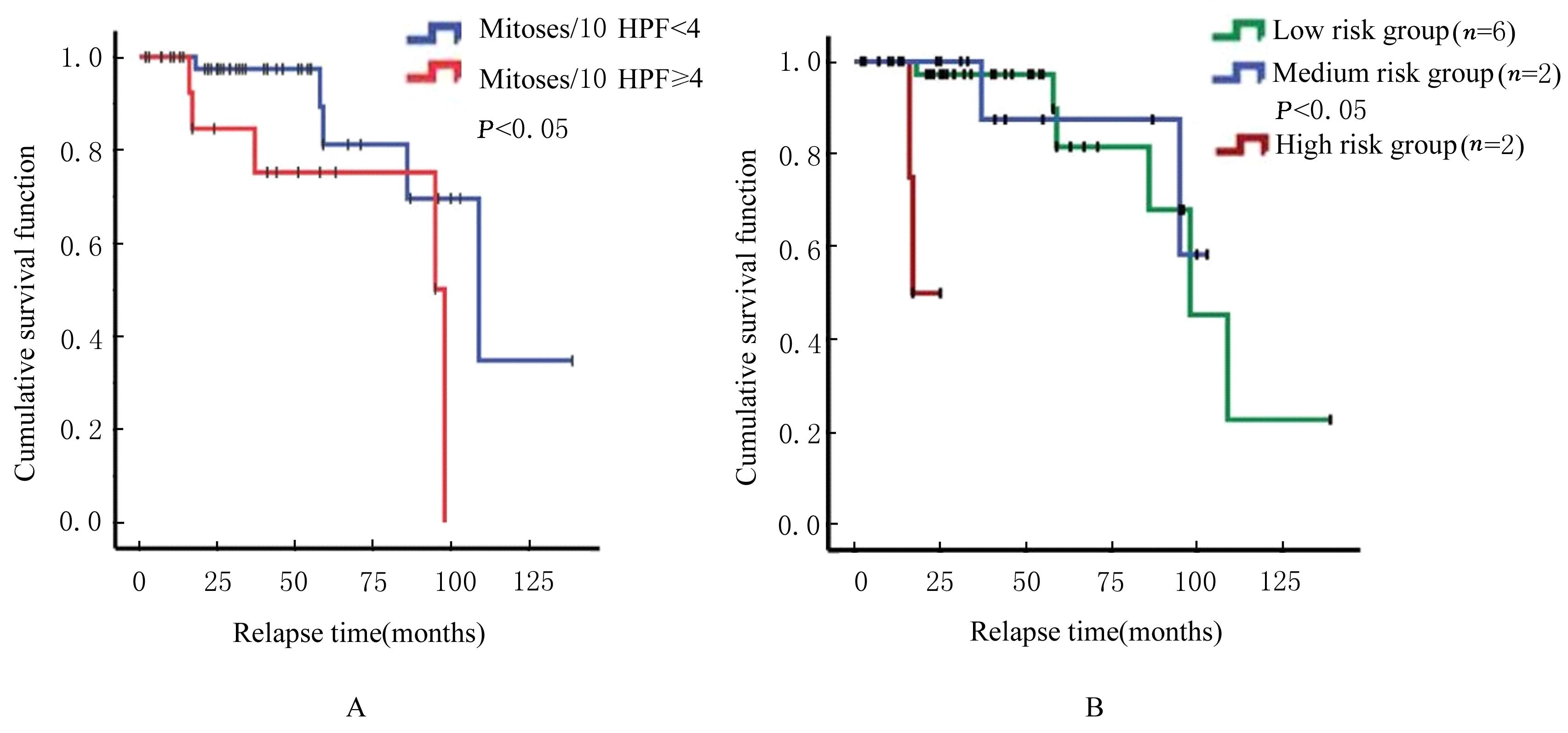
Fig. 4
Analysis on prognosis-related factors of SFT patients detected by Kaplan-Meier survival curve method"
| 1 | KLEMPERER P, COLEMAN B R. Primary neoplasms of the pleura. A report of five cases[J]. Am J Ind Med, 1992, 22(1): 1-31. |
| 2 | GENGLER C, GUILLOU L. Solitary fibrous tumour and haemangiopericytoma: evolution of a concept[J]. Histopathology, 2006, 48(1): 63-74. |
| 3 | ZHANG W D, CHEN J Y, CAO Y, et al. Computed tomography and magnetic resonance imaging findings of solitary fibrous tumors in the pelvis: correlation with histopathological findings[J]. Eur J Radiol,2011,78(1): 65-70. |
| 4 | ZHOU Y H, GONG G H, TANG Y X, et al. Paratesticular solitary fibrous tumor: a case report and review of literature[J].Int J Clin Exp Pathol,2015,8(3): 3358-3361. |
| 5 | ROBINSON L A. Solitary fibrous tumor of the pleura[J]. Cancer Control, 2006, 13(4): 264-269. |
| 6 | BODDAERT G, GUIRAUDET P, GRAND B, et al. Solitary fibrous tumors of the pleura: a poorly defined malignancy profile[J]. Ann Thorac Surg, 2015, 99(3): 1025-1031. |
| 7 | LAHON B, MERCIER O, FADEL E, et al. Solitary fibrous tumor of the pleura: outcomes of 157 complete resections in a single center[J]. Ann Thorac Surg, 2012, 94(2): 394-400. |
| 8 | MOSQUERA J M, FLETCHER C D M. Expanding the spectrum of malignant progression in solitary fibrous tumors: a study of 8 cases with a discrete anaplastic component: is this dedifferentiated SFT? [J]. Am J Surg Pathol, 2009, 33(9): 1314-1321. |
| 9 | ENGLAND D M, HOCHHOLZER L, MCCARTHY M J.Localized benign and malignant fibrous tumors of the pleura. A clinicopathologic review of 223 cases[J]. Am J Surg Pathol, 1989, 13(8): 640-658. |
| 10 | ENZINGER F M, SMITH B H. Hemangiopericytoma. An analysis of 106 cases[J]. Hum Pathol, 1976, 7(1): 61-82. |
| 11 | 王 坚, 朱雄增. 软组织肿瘤病理学[M].2版.北京:人民卫生出版社,2017:318-330. |
| 12 | TANDON N. Solitary fibrous tumor of the vulva: case report of a rare entity and r eview of literature[J]. Int J Gynecol Pathol, 2021, 40(3): 234-239. |
| 13 | 王贞香, 安 琼, 刘雨娟, 等. 肝纤维化中西医结合诊疗临床研究[J].中国实用内科杂志,2021,41(1):2. |
| 14 | SCHWEIZER L, KOELSCHE C, SAHM F, et al. Meningeal hemangiopericytoma and solitary fibrous tumors carry the NAB2-STAT6 fusion and can be diagnosed by nuclear expression of STAT6 protein[J]. Acta Neuropathol, 2013, 125(5): 651-658. |
| 15 | DOYLE L A, VIVERO M, FLETCHER C D, et al. Nuclear expression of STAT6 distinguishes solitary fibrous tumor from histologic mimics[J]. Mod Pathol, 2014, 27(3): 390-395. |
| 16 | YOSHIDA A, TSUTA K, OHNO M, et al. STAT6 immunohistochemistry is helpful in the diagnosis of solitary fibrous tumors[J]. Am J Surg Pathol, 2014, 38(4): 552-559. |
| 17 | KOELSCHE C, B2-STAT6 fusion for the diagnosis of solitary fibrous tumour [J]. Histopathology, 2014, 65:613-622. |
| 18 | TAI H C, CHUANG I C, CHEN T C, et al. NAB2-STAT6 fusion types account for clinicopathological variations in solitary fibrous tumors[J]. Mod Pathol, 2015, 28(10): 1324-1335. |
| 19 | SALAS S, RESSEGUIER N, BLAY J Y, et al. Prediction of local and metastatic recurrence in solitary fibrous tumor: construction of a risk calculator in a multicenter cohort from the French Sarcoma Group (FSG) database[J]. Ann Oncol, 2017, 28(8): 1979-1987. |
| 20 | VALLAT-DECOUVELAERE A V, DRY S M, FLETCHER C D. Atypical and malignant solitary fibrous tumors in extrathoracic locations: evidence of their comparability to intra-thoracic tumors[J]. Am J Surg Pathol, 1998, 22(12): 1501-1511. |
| 21 | HASSANI M, JUNG S, GARZIA L, et al. Aggressive behavior predictors in solitary fibrous tumor: demographic, clinical, and histopathologic characteristics of 81 cases[J]. Ann Surg Oncol, 2021, 28(11): 6861-6867. |
| 22 | DEVITO N, HENDERSON E, HAN G, et al. Clinical characteristics and outcomes for solitary fibrous tumor (SFT): a single center experience[J]. PLoS One, 2015, 10(10): e0140362. |
| 23 | DEMICCO E G, PARK M S, ARAUJO D M, et al. Solitary fibrous tumor: a clinicopathological study of 110 cases and proposed risk assessment model[J]. Mod Pathol, 2012, 25(9): 1298-1306. |
| 24 | GOLD J S, ANTONESCU C R, HAJDU C, et al. Clinicopathologic correlates of solitary fibrous tumors[J]. Cancer, 2002, 94(4): 1057-1068. |
| 25 | ELTAWIL K M, WHALEN C, KNAPP B. Solitary fibrous tumor of the greater omentum: case report and review of literature[J]. Surg Case Rep, 2021, 7(1): 94. |
| [1] | Pengxiang HUI,Xiao YANG,Xu WANG,Ming ZHANG,Haitao FAN,Huikang YU,Yinchun WANG,Qun ZHAO,Gaowen TANG,Ranwei LI. Renal solitary fibrous tumor complicated with hydronephrosis: A case report and literature review [J]. Journal of Jilin University(Medicine Edition), 2022, 48(6): 1593-1598. |
| [2] | Lina SONG,Chunyue WU,Qingyan QIN,Tianshu CHU,Qilin LIU. Familial multiple odontogenic keratocysts:A report of two cases and literature review [J]. Journal of Jilin University(Medicine Edition), 2022, 48(4): 1035-1039. |
| [3] | Wei WANG,Baisong LIN,Haixing LIAN,Xudong GUO,Chen CHEN,Xiuhe ZHANG. Atypical bilocular myxoma:A case report and literature review [J]. Journal of Jilin University(Medicine Edition), 2022, 48(2): 500-504. |
| [4] | Aiping WEN,Le LUO,Zhiwei MENG,Jingji JIN,Honggui ZHOU,Jihong ZHU. Expression of Tip60 protein in endometrial adenocarcinoma tissue and its clinical significance [J]. Journal of Jilin University(Medicine Edition), 2021, 47(5): 1244-1249. |
| [5] | Meisi REN,Yu FAN,Qingrui XUE,Tianyu WANG,Guangxiang ZANG,Hongchen SUN. Alveolar soft part sarcoma of right buccal mucosa: A case report and literature review [J]. Journal of Jilin University(Medicine Edition), 2021, 47(5): 1281-1286. |
| [6] | Qi ZHU,Lamei LI,Yanjun CAI,Fang XU,Junqi NIU,Wanyu LI. Hepatoid adenocarcinoma of stomach:A case report and literature review [J]. Journal of Jilin University(Medicine Edition), 2021, 47(4): 1028-1032. |
| [7] | ZHANG Yiqun, JIANG Weibo, YUAN Sheng, YU Wei. Analysis on follow-up results of postoperative function and recurrence of 23 patients with tenosynovial giant cell tumor in hand [J]. Journal of Jilin University(Medicine Edition), 2020, 46(05): 1061-1064. |
| [8] | BAN Shuofeng, ZHANG Shichen, SUN Yidan, WANG Jing, HAN Bing. Expressions of heterogeneous nuclear ribonucleoprotein D and epithelial cell adhesion molecule in oral squamous cell carcinoma tissue and their significances [J]. Journal of Jilin University(Medicine Edition), 2020, 46(03): 589-593. |
| [9] | LIU Xiuhua, WANG Man, DONG Xinjie, LIU Jingnan, HAN Wei, GUAN Yinghui. Expression of filamin A in cancer tissue of cervical cancer patients and its clinical significance [J]. Journal of Jilin University(Medicine Edition), 2019, 45(06): 1238-1242. |
| [10] | WANG Chuang, YU Shuli, LI Tao, LYU Rongrong, QI Jiemin. Expressions of heparanase and integrin α5β1 proteins in hydatidform mole tissue and their clinnical significances [J]. Journal of Jilin University(Medicine Edition), 2019, 45(06): 1361-1366. |
| [11] | LI Hua, CAO Yansha, ZHAO Jinping, REN Fu, LI Ning. Expression of SIRT6 protein in colon cancer tissue detected by tissue microarray technique and its clinical significance [J]. Journal of Jilin University(Medicine Edition), 2019, 45(04): 893-898. |
| [12] | DUAN Jiqing, SUO Jian, SUN Donghui. Application of two-step procedure to turn rectum out from abdominal cavity in radical resection of low rectal carcinoma by natural orifice specimen extraction surgery: A report of 39 cases [J]. Journal of Jilin University(Medicine Edition), 2019, 45(03): 683-687. |
| [13] | TIAN Yanhua, SU Kai, WANG Sanchun, TONG Weifang, ZHANG Xu, WEI Mingxue, FENG Qingjie. Sarcomatoid carcinoma of throat: A report of 5 cases and literature review [J]. Journal of Jilin University(Medicine Edition), 2019, 45(03): 697-700. |
| [14] | MU Tianchi, LIU Chao, FU Shuai, LI Qiyang, WANG Xinmeng, XIAO Jianying. Expression of activator of basal transcription 1 in gastric cancer tissue and its clinical significance [J]. Journal of Jilin University(Medicine Edition), 2019, 45(01): 94-99. |
| [15] | LI Hongxia, GONG Haiye, ZENG Xiao, ZHANG Susu, LIU Bofeng. Expressions of TGF-β1 and PLGF in tissue of patients with different types of gestational trophoblastic diseases and their significances [J]. Journal of Jilin University(Medicine Edition), 2018, 44(05): 1041-1046. |
|